










(Continued from Part 1. This concludes the article.)
An Aside: Please, take note of the last photo in Part 1 of this article. See how one end has a dark clippy thing, and I affixed the lanyard loop to the other end? Well, should you desire to recreate my own experience on your own, please, please, please do NOT simply open the package of your shiny new razor knife, and then drop it into your medic kit. It turns out that, when I was doing some chore or another in my well-lighted, warm, very own basement, I learned that the blade (you know: that sharp thing!) protrudes from the handle AT THE END TO WHICH I HAD AFFIXED MY LANYARD LOOP! (a) If you do not learn that, at your leisure, you may learn it, abruptly, in the dark, in the rain, on your very own emergency scene. And, you may wind up contributing your very own blood to the bodily fluids present on scene.
Most of us might find that distracting.
TDW-Mark II has observed, in the past, when I have lacerated myself, “Oh! You are on blood thinners! You are really gonna bleed from that!” (a) I KNOW that I am on blood thinners, a fact about which my cardiologist has waxed most eloquent, and (b) having been an RN for generations nearly beyond number, as well as a paramedic and a midlevel practitioner, I believe that I am familiar with the effect blood thinners have upon coagulation, and (c) as well as the effects of lacerations interacting with the foregoing. But, thank you very much.
So, for love of Pete, manipulate your kit’s contents in the warmth/light/safety/comfort of your own home, in order to AVOID recreating my own fail (or near fail, depending upon which part of this epistle has had the most impact upon you).
Then, of course, there is the “Summer In The Trenches Of The Somme” test Aesop suggested we consider. The PVC pipe idea has many advantages, particularly given Commander Zero’s initial epiphany ref his bicycle kit.
Plastic Ammo Cans
I noticed, when my boys were scouts, and, as Assistant Scoutmaster I was de-facto medical officer, that several manufacturers make 50 cal “fat boy” ammo can copies in plastic, with considerable attention paid to the issue of weatherproofing the seal. There is a compression latch, and an “O” ring to seal the lid to the body of the case. I purchased one, and stocked it as the “House Kit”. I wove a “tamper evident seal” through the latch, so that it is (surprisingly) evident when someone has entered the kit, and thereby trigger an inventory. The kit in my home is a copy of the set up I created for the scouts, with a packing list identical to my vehicle bags.
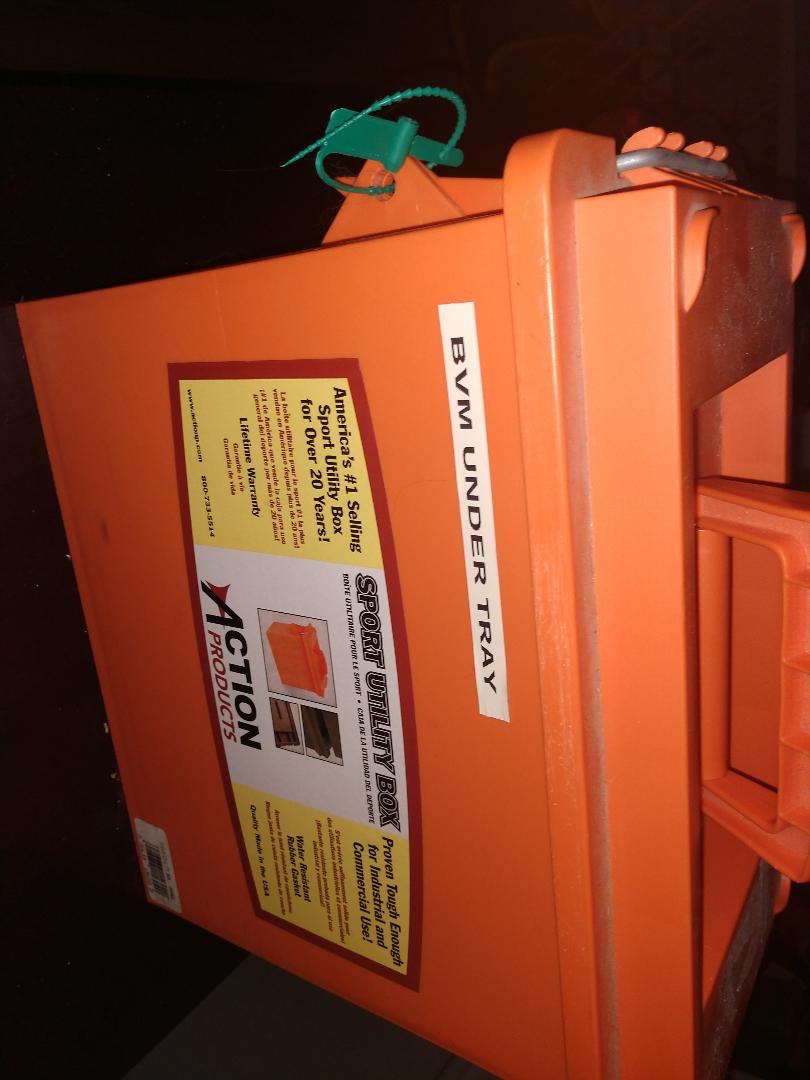
Picture Seven: Note the “tamper evident seal” on the left side of the box. Entry will not happen, without destroying the tag. Please note that, presently, the BVM (and the matching Pediatric BVM) are not in the box, but, rather, in a plastic bag immediately adjacent, and secured to, the box. (Dagnabit! Gotta update the labeling of my box!)
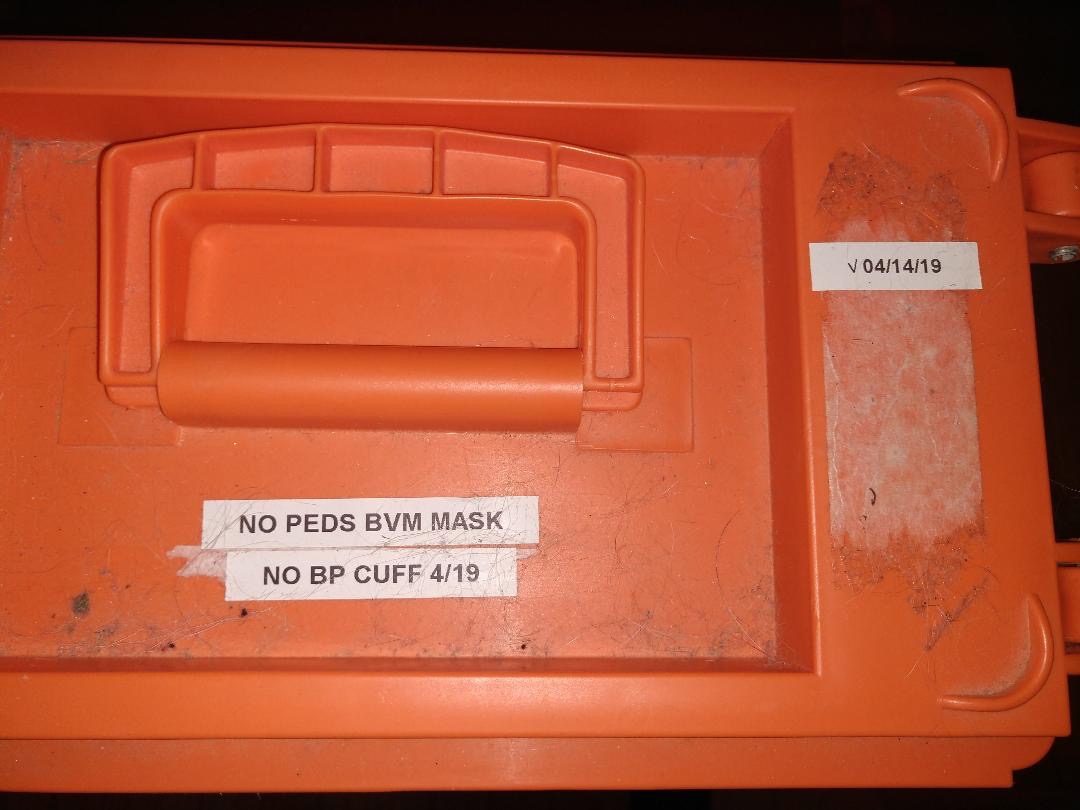
Picture Eight: When I last repacked this kit, the pediatric BVM (manual resuscitator) mask was stiff and would/could not effect a seal. A new one just arrived (with 2 more in my “emergency restock reserves”, here at Camp McFee) Similarly, the BP cuff was found to have a dry rotted bladder, and would not hold air. The replacement is on my shopping list, but, alas, The Overtime Fairy has been occupied in other precincts, and has not seen fit to visit me. Another entry on the “Gotta replace this stuff!” list. Darned Overtime Fairy! You may have noted that I noted the date of my last inspection, along with priority deficiencies found at that time. December found me replacing the peds mask, and that’s ANOTHER label, that I have to update!
The red bags in our vehicles lend themselves to directing associates. Relevant little tale: This no stuff, there I was one day, fighting disease and saving lives in the urgent care that employed me, and this child of God arrived, markedly dyspneic. (short of breath. VERY short of breath!) Since I knew (a) that my kit had been inspected, and (b) by whom, therefore (c) it appeared to be reasonable to toss my car keys to one of the MAs, and suggest that a quick field trip to my vehicle trunk, and retrieval of my medic bag, would make me feel warm and fuzzy all over. Like, right now, please.
Due to the fact that I squirrel away lotsa stuff in my trunk, well, the redness of the medic bag does help it stand out from the other supplies hidden therein. She returned, promptly, with my bag, and I retrieved my BVM, and staged it on the counter in case of need. Said need did not develop, thankfully.
This might be a good place to mention coordinating reserve stocks, and their outdates. Once I get this synchronized, I will be buying new, say Quick Clot, something like 6 months before I have to buy new, say, battle dressings. Larger capital expenditures, like BVMs or BP cuffs, will, ideally, be offset by several months from cash flow hemorrhage dates like auto insurance payments, or Christmas, or, really, the first six months of the year, before I hit our health insurance deductible amounts.
Although, should I never hit our deductible amounts, I would see that as a multiple layer win.
Other Kits
We also have smaller “camper kits”, in each in each vehicle as well as one in our camper. These are directed to both smaller scale ouchies, being primarily “boo-boo kits”, as well as family-friendly OTC medication sources. In “snack-sized” zipper seal bags, I have a dozen doses of acetaminophen (pain reliever and fever reducer), lomotil (anti-diarrheal), famotidine (antihistamine, employed most often as an antacid), diphenhydramine (antihistamine, employed most frequently, amazingly enough, as an antihistamine for itching as well as allergies. Also makes you sleepy). Finally, I have some cetirizine to moderate sniffles due to allergies (antihistamine, less sedating).
On each bag I identify the medication, note dosing instructions, date packed (each year sees the meds turned over due to effects of heat/cold), and expiration date. I also note the lot number in event of recalls. You might elect to write these notes on an index card, and enclose it in with the meds.
I upgraded the wound care section, as these began life as “Big Box Store First Aid Kits”. I added larger Bandaids, and more 4 x 4 sterile gauze. I double bagged the instant ice pack included in each kit, so as to try to limit how widespread the mess will be should a bag develop a leak. On the outside I noted the date of check and repack, updating the note at each recheck, every 6 months or each year.
So, in the spirit of thoroughness, our “camper kits” have been upgraded. The items that might be damaged by wet, have been sealed.
ADVERSE EFFECTS
In medicine, we contemplate risks and benefits, and attempt to prescribe interventions that we anticipate will have more likelihood of benefit than risk. Alternatively, we seek adverse consequences that are tolerable, or at least dwarfed by the anticipated benefits. (like antibiotics, which may produce diarrhea, in exchange for treating your infection before it becomes life or limb threatening)
Therefore, let me share another lesson learned: Not so very long ago, I was helping my daughter and her family move. I was carrying a load of boxes to the trailer, and scraped my leg on the edge of the trailer. I did not think too much about it, scrape, no big deal, right?
Later observation revealed swelling about the injury, with palpation revealing that this was a collection of fluid, most likely blood. I cleaned up the scrape, applied a gauze pad, and went to bandage it with the Coban that I had vacuum sealed.
So, about that…. It was revealed to me that, when you vacuum seal Coban, you have compressed it. When you have compressed Coban, particularly for any length of time, it melts together into a solid, gummy mass, with no discernible end to pick off so as to unroll it so you could, you know, USE it. This is in addition to the fact that the two rolls imaged herein, appear to have been welded together, such that TDW-Mark II proved unable to reef one from the other.

Picture Nine: Congealed Coban
That is kind of unhelpful.
Fortunately, my son in law is not so afflicted with OCD as I am, and had Coban, that he had not vacuum sealed, and so he provided me with un-gummed Coban with which to bandage my injury. Back to work!
Let me reference the above-mentioned fail, of initially securing my lanyard loop on the pokey end of the retractable razor knife. Fortunately, there was no blood letting to reveal the depths of my failure, but, please, learn both lessons from my experience. First, identify the pokey end BEFORE handling the knife. Secondly, handle and manipulate your stuff in the warmth/light/quiet of your own home, BEFORE you feel compelled to do so at night, in the cold, and/or in a wind. On an injury scene. Surrounded by excited and unprepared folks. And feeling time pressure because somebody is hurting.
About The Author:
“Skyrat” is the pen name of a Mid-Level provider in a clinic in Fly Over Country. He has been an ER RN for more than 30 years, and an EMT for a large city fire department. He is an Amateur Radio Operator, shooter, and camper.
Skyrat, thank you for the article, it is very helpful! While I am not a medical professional, I live on a farm and I am constantly give 1st aid to someone or some animal. How often should some of these items be replaced (like quick clot)? Will placing some of these item, like a BP cuff, in ziplock bags extend their usage? What causes them to deteriorate so quickly, just age or heat? I use a lot of Coban; does it last longer if stored in ziplock bags?
The issue with stored Coban is heat and presseure, kind of like explosives but without the exploding. Ziplock bags I feel are fine for them and have had no issue with storing them that way. Quick clot has a best by date on it. I don’t like to use it but that is personal preference and nothing against it. As for the BP cuff I don’t have a solution for that because I use an electronic solution. Not as good as a dedicated device but in a situation I would use my kit we are just beyond taking vitals. I am also not a medical professional so with anything I say YMMV.
Animal House: ref the Quick Clot: the hemostatic agents (including Celox) have outdates on the packaging. Being an old nurse, I cycle the “past expiration date” material to my “training” box. First use is to train (surprise!) with the out dated stuff, rather than the fresh items.
Secondary use, is if TSHTF, I would have supplies that might be useful. That is, MIGHT be useful, in a “Zombie Apocalypse” sort of scenario.
I bagged the Coban, so as to keep it in one place. Otherwise, it tends to migrate beneath other stuff, and therefore requires digging around to find/extract it. The vacuum pack was my OCD kicking in, and was a horrible fail. As Just Some Guy notes, zip lock bags are suitable.
Ref the BP cuff: rubber goods, like bladders, simply “age out”. While it takes some time (the subject BP cuff bulb was originally acquired circa 1975), it should be expected (and planned for. Now, THAT is another imperfection in my planning!) Recognize that the electronic BP measurement devices, likely still have a rubber (or rubber like) material forming the bladder that applies the pressure, so it is a good idea to anticipate that material dry rotting, and what you will do to replace it when it does.
Great article. I’ve been an EMT on and off for 30 years, mostly while I was a cop in the ESU, and a former volunteer firefighter. The rotation of EMS supplies is a constant but necessary chore. You’re clearly on top of it! Thanks for writing the article.
Speaking of Medical equipment-
(Please disregard my previous incorrect link.)
https://mostlycajun.com/wordpress/?attachment_id=48665
We need more on this topic! Because radio and medicine are the two weakest skill sets that sorely need to be addressed. Radio would be the easier topic to get an handle on, and because it is essential to our security, it is the priority, then comes first aid, or in some cases, ‘last-aid’. When is come to gun shot wounds, it is all about stopping the bleeding. It will likely become septic, and the only chance to mitigate that would be oral antibiotics immediately, when huge doses of IV antibiotics are called for.
As some one who took blood thinners for years, before I stopped taking medications of all kinds, the bleeding from a small cut was difficult to stop, and a scary situation. If taking blood thinners, I would be prepared to use a tourniquet. If in the middle of a war zone, the risk of bleeding out is high, therefore in my unqualified opinion, the possible benefit from blood thinners is for myself, inferior to the risk of bleeding out due to a minor laceration, and certainly in the event of a gun shot wound.
I would discuss this with your doctor. Unstable angina posses certain risks, and requires the use of blood thinners. Stable angina is different. However, consider that it would safer for the Doctor to avoid potential lawsuits, and so would naturally insisted on the use of a blood thinner.