(Continued from Part 1. This concludes the article.)
Things to consider beyond bleeding
No matter how good you are at stopping a hemorrhaging blood vessel, you or someone that you designate must call 9-1-1 right now! Don’t say “Somebody call 9-1-1!” Bob may think that John will call; John thinks that
Bob is calling – and no one calls. Instead designate: “John, call 9-1-1!” If you are faced with more than one victim, which might occur in a motor vehicle accident, decide as quickly as you can where the worst bleeding is occurring – which person and which part of the body. Unless you have extensive medical training in the management of trauma that will be an exceedingly challenging task. Accept the fact that you probably won’t do everything right. But whatever you do will make a difference.
Anticipate that the person whose bleeding you have managed to stop will be likely to go into shock – a condition in which blood pressure falls and the diminished output of the heart causes multiple organs to fail. It is often fatal. It is characterized by weakness, pale, clammy skin, a rapid pulse, rapid breathing, anxiety, and confusion. Elderly persons are most at risk and need to be observed closely. Although first aid manuals advise keeping the victim warm it’s important not to cover bleeding wounds.
A compound fracture, a broken bone whose fragments protrude through the skin, is likely to include one or more torn blood vessels. Pressure and packing may not be possible without causing further injury, and placement of a tourniquet is the first step if there is significant bleeding. In doing so take particular care not to move the extremity in order to avoid damage to nerves and further damage to torn blood vessels. When emergency responders are only minutes away, wait for them to splint the extremity for transport.
Save that finger! Rapid transport of trauma victims and the ability to reattach body parts is one of the triumphs of modern medicine. A severed finger should be wrapped in a damp paper or cloth towel, placed in a ziplock
bag or similar container and sent to the emergency room with the owner. The bag with the finger can be placed on ice, especially if it will take more than a few minutes to reach the hospital but ice should not come in direct contact with the digit. Never use dry ice. Saving a larger body part such as a foot or hand is beyond the scope of this article.
Never do anything for the first time. Training is crucial.
My brother, a former law enforcement officer, shared some wisdom that I have never forgotten: “Never do anything for the first time,” meaning that you should practice every anticipated scenario, at least in your mind
if not live. Every student in my Stop the Bleed class is required to use pressure and packing on “Stumpy,” a training device that simulates a human thigh that has sustained a deep stab wound and a 9-mm entry and exit wound. Each student applies the tourniquet to my upper arm and cranks the windless as far as possible. If they don’t do it perfectly the first time, they must do it again. Yes, it’s really painful but they quickly realize that applying a tourniquet to a real person is harder than it looks and by doing it on a live person it helps them to move through their fear.
Caches, caches everywhere. What you need in order to apply what you have learned.
Not one Stop the Bleed kit, but several. At minimum you should have a kit wherever you might need it: your home, your office and each vehicle. You will need one for your boat or RV.
Prepare for the worst case. A single tourniquet for each kit is not enough. The Rawles mantra of “Two is one and one is none” takes on special meaning here. Think in threes. You will want a spare if the windlass breaks,
as plastic ones sometimes do, but there are two more compelling reasons. You might need a second tourniquet if the first one does not stop the bleeding, as noted above. There might be another source of hemorrhage, or perhaps a second victim.
Tourniquets usually arrive wrapped in plastic, which in your adrenalin-fueled state with deteriorating fine muscle control will be maddeningly difficult to remove. And that’s not all. You should extend the tourniquet, undo the tab that the manufacturer threaded through a latch, re-fold it and hold it together with a rubber band. That makes it easy to have it at the ready when you must place it around the upper thigh or the upper arm. Trying to slide an already looped band over a bloody, mangled foot or hand is a slow, messy process and wastes precious seconds.
Do you need a clotting agent such as QuikClot or a pressure dressing/Israeli bandage? The farther you are from emergency services the more likely you will need these in each Stop the Bleed kit. If you are on a hunting trip, at a remote campground or miles from shore in your classy but slow sailboat, these items can be lifesaving.
Addenda
The Red Bag
 [1]We have developed “Red Bags” for placement in our church where rescuers can access them within moments by our own emergency response team. More than two dozen members of the congregation have committed to step in as soon as the scene is safe to apply the bleeding control principles described in this article. All are current or former healthcare workers or law enforcement personnel or have received training in advanced first aid.
[1]We have developed “Red Bags” for placement in our church where rescuers can access them within moments by our own emergency response team. More than two dozen members of the congregation have committed to step in as soon as the scene is safe to apply the bleeding control principles described in this article. All are current or former healthcare workers or law enforcement personnel or have received training in advanced first aid.
There are four Red Bags on our campus in two separate buildings. They have been placed at opposite ends of each structure in case one or the other cannot be reached because of a dangerous situation. That is exactly what happened during the Tree of Life massacre in Pittsburgh on October 27th, 2018. All their supplies were in one location. Another poignant reminder that “two is one and one is none.”
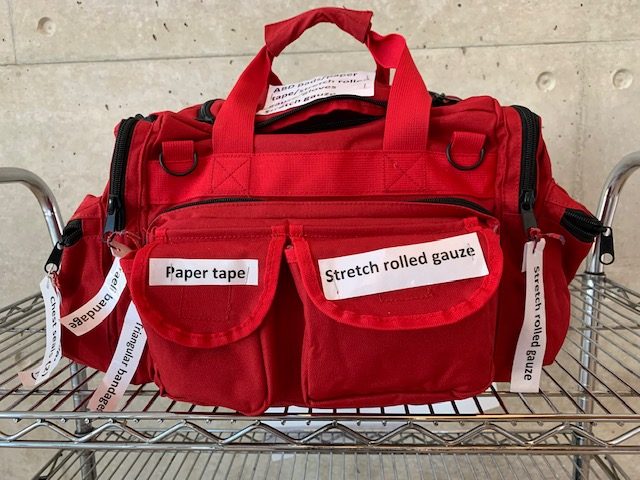
Stop the Bleed kits are available from a variety of sources but the Red Bag, of which we have four, is inexpensive and has enough supplies to treat several victims. They contain the basic materials needed to control hemorrhage in the early minutes of an incident: rolls of gauze, ABD and gauze pads, triangular bandages, tourniquets, Israeli dressings and paper tape. A standard First Aid cabinet contains minor supplies such as Band-Aids, small gauze pads, antibiotic ointment and tape. Each bag contains two chest seals but does not contain needles for decompression of a pneumothorax. Needle decompression of a tension pneumothorax is beyond the scope of this article. Remember that a gunshot may leave both an entry and an exit wound, and thus you may need to apply two chest seals.
Our Red Bags do not contain QuikClot clotting gauze or similar hemostatic agents designed to hasten the clotting process. Your circumstances, such as distance from a medical facility or first responders, may require that these should be added to your Stop the Bleed kit. Note that this technology continues to evolve and materials that were in use only a few years ago have been replaced by newer agents.
The contents of each pocket of the bag are prominently labeled for rapid access. Web loops on the back of the bag hold six pairs of scissors. (The last thing you need to hear when multiple victims have been injured is “Who has the scissors?”)
Your needs may differ
The contents of our Red Bag are intended for rescuing victims during the few minutes before the first 911 responders arrive. (The time required for an ambulance response ranges from four to ten minutes in urban and suburban areas, with very wide variation.) More remote scenarios require
materials and instruments such as chest seals with valves, one or more chest decompression needles, extremity splints, Mylar blankets, IV fluids and accessories, hemostatic gauze, etc.
Where to get Stop the Bleed Training
The Stop the Bleed [2] website provides a description of the program, its history, information regarding training venues, Stop the Bleed kits and training supplies. Nearly every large medical center in the country now has Stop the Bleed training programs. Many offer them at no cost. The American Red Cross and the American Heart Association offer training and you will find other venues on the Internet.
From the SurvivalBlog Archives:
Letter: Stop the Bleed training by Hugh James Latimer, May 25, 2017
Introduction to Tactical Combat Casualty Care by W.H., August 22, 2014
A SHTF Guide to Mass Casualty Incidents by W. G. Curry NRP,TP-C September 29, 2015
Letter re: Wounding Patterns August 8, 2016
Some IFAK (Individual First Aid Kit) Facts, parts 1 and 2 by MtnDoc in Washington, July 30-31, 2019
Further reading
Tobias AZ et al., Tree of Life Synagogue Shooting in Pittsburgh:
Preparedness, Prehospital Care, and Lessons Learned, Western Journal of
Emergency Medicine March 2020, Volume 21, No. 2. This article shows how community and individual preparedness saves lives. It also points out two easily correctible errors: failure to check equipment and inadequate positioning of supplies. There are several useful concepts that might apply in a TEOTWAWKI scenario.
Turning bystanders into first responders, The New Yorker Magazine April 1, 2019: 480 seconds (YouTube) A realistic video of a workplace shooting, YouTube August 22, 2019
Also see: www.trauma-news.com Updates on bleeding control
About The Author
Philip J. Goscienski, M.D. is a retired pediatric infectious diseases specialist and retired Captain, Medical Corps, U.S. Navy. He has written more than 700 newspaper and magazine articles, four books and several medical journal articles. Since 2001 he has been the medical director of the CPR program at his church and has trained more than 700 of its parishioners in CPR and has trained more than 100 members of that faith community in Stop the Bleed. You may contact him through www.stoneagedoc.com [3].